Chronic Pelvic Inflammatory Disease
The
correlation between PID and chronic pelvic pain has been known for some time
and has been confirmed by a study published by Buchan
et al in 1993. Such patients were 10 times more likely to develop pelvic
pain or an ectopic pregnancy and were 8 times more at risk of having a
hysterectomy. This was more common with moderate or severe pelvic adhesions [Eschenbach et al, 1997] but especially so if these
adhesions involved the ovaries or restricted uterine or tubal motility [Beard and Dias, 2001].
Different organisms can cause pelvic
inflammatory disease and most of these cases are sexually
transmitted. However, in 10% of the cases infection may follow invasive
diagnostic or surgical procedures. There is also an increased risk of PID
during the first 3 weeks following IUCD insertion [Farley et al, 1992]. Accordingly, there is some evidence
to screen for chlamydia before IUCD insertion [Prodigy Clinical Guidance, April 2003], as it is currently the most important sexually transmitted microbe.
Women under the age of 25 years are at greater risk to PID in general as
those with multiple partners and those not practising safe sex. In most cases
it is a silent infection or may cause minimal discomfort. However, it can present with vaginal discharge, painful urination, pelvic pain and
intermenstrual vaginal bleeding. The late outcome of untreated chlamydia
infections will be chronic pelvic pain, infertility and increased risk of
ectopic pregnancy. It is important here to stress the difference
between upper and lower genital tract infections in this respect. Upper genital tract infections are 7 times more likely to cause pelvic pain
than lower genital tract infections. It is also important to remember that
serological tests for chlamydia do not differentiate between the two.
Recently more emphasis has been directed towards
regular screening for early detection of chlamydia infection to prevent
complications. As women under the age of 25 years are at greater risk, they
should be targeted for annual screening [Prodigy
Clinical Guidance, April 2003]. Older women may have similar screening
if they had multiple partners. Retesting is advisable 3 - 4 months after
finishing treatment especially in adolescents and for women with untreated
partners. Opportunistic screening can be done in sexual health, family
planning, gynaecology and early pregnancy clinics. A good number of female patients accepted to
be tested (80%), and reports of 6-10% positive results were confirmed in 16-25
years old women. Alarmingly 70% were asymptomatic. To reach a wider population
base, postal testing kits have been used [Ostergaard
et al, 2003]. Other organisms that can cause
pelvic inflammatory disease include:
- Niesseria
gonorrhoea
- Mycoplasma
hominis
- Ureaplasma
urealyticum
- Bacteroids
Pelvic
inflammatory disease can be polymicrobial caused by multiple rather
than a single organism. Furthermore, in many
cases organisms isolated from the vagina or cervix may not be
responsible for the PID episode in question. Nevertheless, in all cases high
vaginal and endocervical swabs are taken automatically for microbiological
analysis. The initial antibiotics course may not be effective in up to 15% of
the cases as treatment is usually started before any reliable bacteriological
culture results are available. This is usually done according to the prevalent
microbes isolated in that society. These factors as well as the patients life
style and failure to identify and treat male partners in many cases can partly explain why 25% of PID attacks are usually recurrent. Accordingly, two
of even three antibiotics are now used, one of them to cover chlamydia
infections. The long-term effect of these infections on the fallopian tubes and
surrounding peritoneum depends on their number, severity and how adequately
they have been treated. Tubal damage and pelvic adhesions may lead to
blockage and future infertility problems, ectopic pregnancies and chronic
pelvic pain. The reported risk of infertility after 1, 2, 3 or more infections
was 11.4%, 23.1% and 54.3% respectively [Westrom and
Mardh, 1983]. Furthermore, with previous history of PID the risk of
ectopic pregnancies was estimated to be 7 times the normal rate [Westrom et al, 1992]. This
was confirmed by epidemiological studies which showed a peak in the incidence
of ectopic pregnancy 15 years after a peak in the incidence of salpingitis [Bjartling et al, 2000].
With
PID, local tissue inflammation and thin peritubal adhesions may form after
chlamydia infection. In some case, the only damage may involve the tubal
mucosa. However, with repeated or severe infections including those caused by
multiple organisms, thick pelvic adhesions or even an amalgamated adnexal mass
can be seen. Omental adhesions are especially common to seal the infection
off the rest of the peritoneal cavity. However, acute pelvic inflammatory disease does not usually show any
characteristic pictures on transvaginal scan examination. Nevertheless,
occasionally increased tubal wall thickness due to oedema and free fluid
with floating particles in the pelvis can be detected. Furthermore,
hyperaemia of the inflamed tube may lead to increased vascular markings on
colour Doppler mapping. In severe cases oedematous intratubal folds on cross
section scanning can show a cogwheel appearance of a thick-walled
multilocular pelvic mass with echogenic fluid collection. On the other hand,
patients with chronic pelvic inflammatory disease may show dilated tubes
with thin or thick walls and atrophic mucosal folds. Cross sectional views of a thick wall
dilated tube may show the 'beads on a string' sign. On the other
hand, incomplete intratubal septae can be seen in acute as well as chronic
salpingitis. Gentle movement of the probe in different directions helps to identify them as intratubal folds projecting into the lumen, but not reaching
the opposite side. However, the most common ultrasonic findings in chronic
salpingitis are thin wall hydrosalpinges, beads on a string
appearance and incomplete septae. For clinical reasons, it is always important
to differentiate a tubo ovarian complex which needs antibiotics treatment from
a pelvic abscess which needs surgical drainage as well. The ovary and tube
can be seen separately during scanning a tubo ovarian complex, which is not
usually possible in most cases with a pelvic abscess.
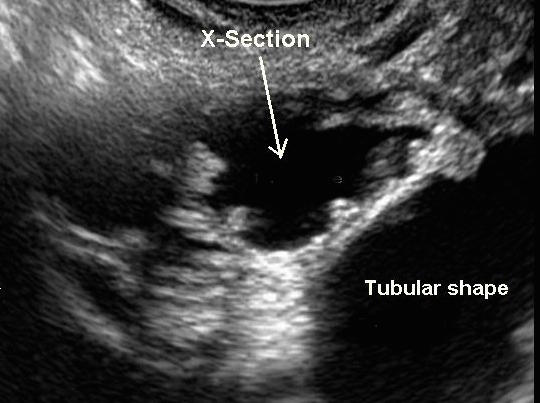
- The first ultrasound image above shows a cross section and tubular parts of a dilated fallopian tube. The cross section shows thick folds which is a sign of acute inflammatory process (acute salpingitis). The x-section pattern is called Cogwheel Appearance.
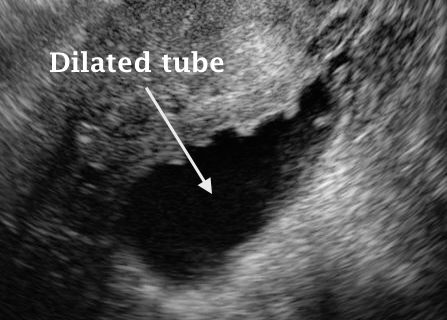
- The second image above shows a dilated fallopian tube with small atrophic folds, diagnostic of chronic salpingitis. The appearance is called Pearls on the String
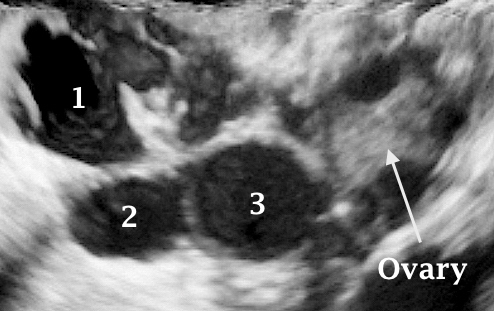
- The third 3D image shows a tubo-ovarian complex, made of the ovary, cross section of a fallopian tube and some peritoneal fluid with thin adhesion folds. Unlike tubo-ovarian abscesses, all structures are clearly and separately identified in this case.
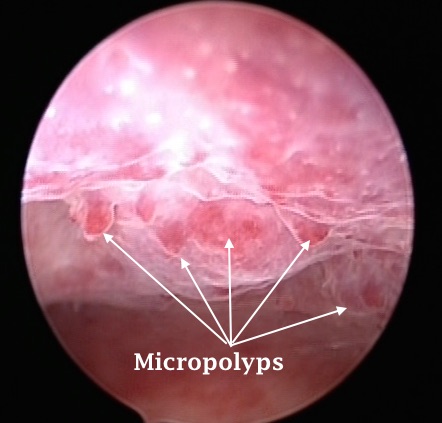
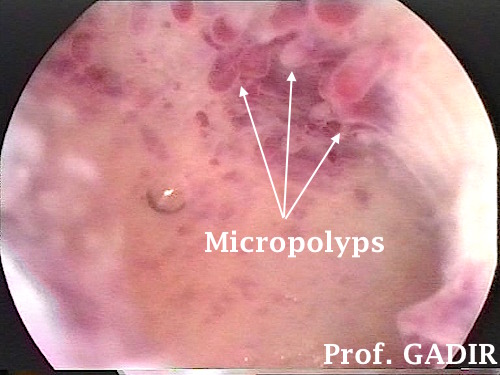
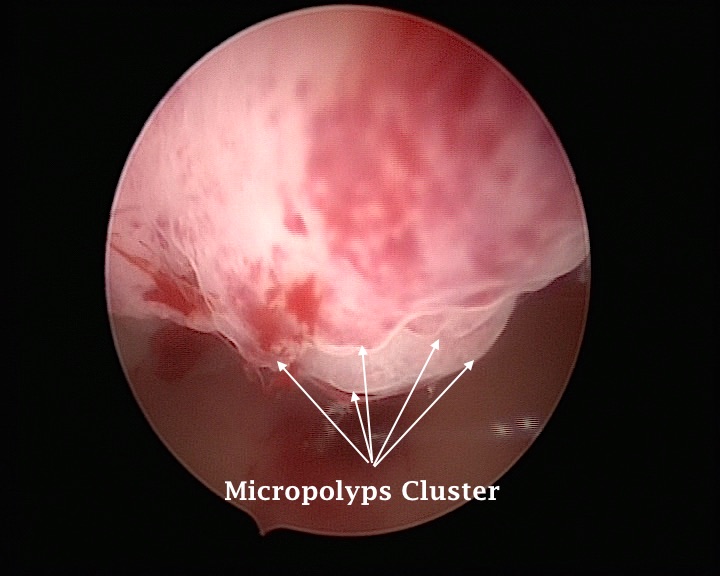
Both laparoscopy and hysteroscopy may show sign of chronic pelvic infection. Micropolyps have been described as a sign of chronic endometritis by Ettore Cicinelli et al in 2005. They present as small projections of 1 mm off the endometrium surface, either singularly, or mostly in small groups. Each one is made of a central blood vessel, covered by some thin layer of stroma tissue and outer endometrium. They are not well seen by transvaginal ultrasound and may show as focal lesions on on side or the other of the endometrium.
The three hysteroscopic images shown below belong to three different patients who presented with pelvic pain and abnormal uterine bleeding. In all cases punches of micropolyps were seen, diagnostic of chronic endometritis. Such picture gives more bleeding than pain, unless combined with inflammatory involvement of other parts of the pelvis. In my experience gentle spiral curettage of such polyps under intravenous antibiotics, followed by at least one week of such medication, controlled the bleeding and helped with pregnancy in few cases who were infertile before.
The role of laparoscopy in the diagnosis of chlamydia infection is not as specific as DNA testing for the microbe. However, pelvic and perihepatic adhesions can be seen.
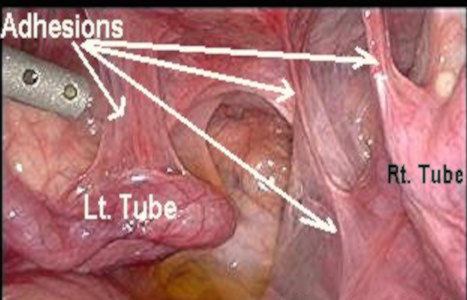
- The first laparoscopic image shown below demonstrates pelvic adhesions following
chlamydia infection. Both tubes and ovaries were involved, and the left tube is
showing a hydrosalpinx.
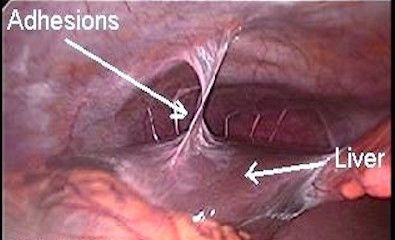
- The second picture shows violin string adhesions
between the liver and the anterior abdominal wall caused by chlamydia
perihepatitis infection [Fitz-Hugh-Curtis Syndrome]. Such perihepatic infection and adhesions can cause acute or recurrent sharp pleuritic upper right quadrant pain and may be
seen in 10-20% of all pelvic infections caused by chlamydia, as reported by the British
Association for Sexual Health and HIV in February 2005. A
high figure of 30% has been reported by Sharma et al [2002]
in patients with chronic pelvic pain compared to 16% in patients who had
infertility investigations at the same time. Liver function tests and
transabdominal scan examination of the liver and perihepatic area are usually
unremarkable. However, CT scanning may show an enhanced hepatic capsule
during the acute phase, but this usually resolves after treatment with
antibiotics [Nishie et al, 2003].
The presence of pelvic adhesions as a cause of pain has been challenged over the years. This in my mind is mainly due to the fact that the background cause which lead to the formation of adhesions in the first place has never been addressed in the same equation. Accordingly, two questions still remain to be answered and these will be discussed in the chapter dealing with pelvic adhesions shown in the side menu.
- Do adhesions cause chronic pelvic pain?
- Is adhesiolysis effective in relieving chronic pelvic pain?