Adhesionsare bands of scar tissues connecting different organs following different types of tissue injury including surgery, infection and endometriosis. In many cases adhesions are discovered by chance during diagnostic laparoscopy. However, most cases of reported adhesions have been seen in women with chronic pelvic pain with or without other pathologies. The site, extent and type of adhesions might affect their mode of presentation. Small bowel adhesions are more likely to cause obstruction symptoms as they could restrict the movement of intestinal contents and cause painful distension of bowel loops. On the other hand, thick adhesions were thought to harbour more neurovascular bundles which could be stretched during certain types of movements leading to chronic pains. However, no correlation was found between the number of nerve fibres within adhesions and pelvic pain. Furthermore, no correlation could be found between the severity of adhesions and the magnitude of pain. [Steege JF, 1994]
From the treatment point of view adhesiolysis has not been shown to cause long-term relief from chronic pelvic pain [Steege JF, 1994] and second look studies showed recurrence of adhesions following surgery. Consequently, its role in the management of chronic pelvic pain is still controversial. However, Peters et al, [1992] showed anexception with bowel adhesions to the anterior abdominal wall. Removing such adhesions was effective in treating chronic pelvic pain. Accordingly, one should take into account the sites and organs involved with adhesions and the pathology which had lead to their formation in the first place. Examples of such conditions include chronic appendicitis, endometriosis, chronic pelvic inflammatory disease and previous surgery.
Occasionally transvaginal scan examination can give some clues to the presence of pelvic adhesions including:
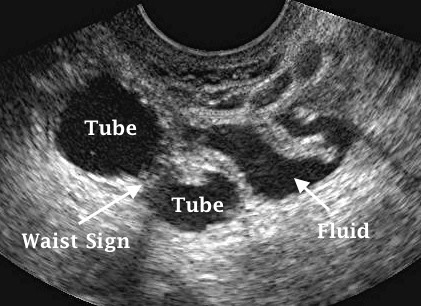
Encysted fluid in the pelvis in the form of peritoneal pseudocysts following surgery or pelvic inflammatory disease may be seen. Unlike free fluid, such cystic areas do not usually change shape significantly during examination as they are enclosed within fixed confinements.
Fallopian tubes can be seen as retort shape fluid filled structures beside the uterus.
Communicating hydrosalpinges are best seen at the middle of the cycle as they drain back into the uterus after ovulation, due to the progesterone induced relaxation of the tubo-uterine junction after ovulation.
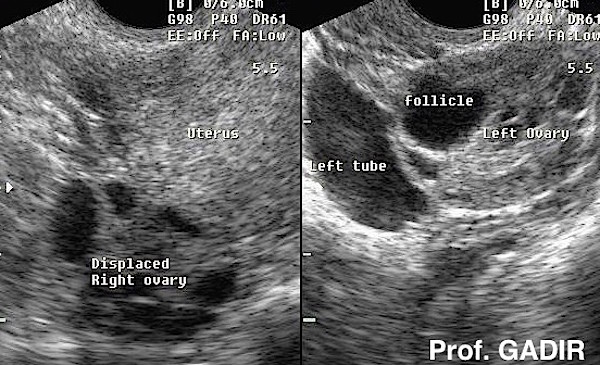
Ovaries dislocated from their usual site between the uterus and the internal iliac vessels may be difficult to see transvaginally. This is especially so if an ovary is stuck high behind the fundus of the uterus. However, such dislocation can be coincidental and the ovary may be seen in its normal position in a follow up scan.
Negative organs sliding sign may be elicited when pelvic organs are stuck together, the uterus and ovaries move freely against each other and relative to the pelvic sidewall, when pushed with the vagingal probe. This may not be the case in the presence of adhesion and all organs move together in the same direction.
Flapping sail sign as shown by bands of thin adhesions moving from one side to the other during movement in the vaginal probe, especially in the presence of fluid in the pelvis.
The first ultrasound image shown above illustrates a dislocated right ovary, lying behind the uterus with the left ovary easily accessible during transvaginal scan examination. The patient presented with deep dyspareunia and secondary infertility.
The second image shows encysted fluid in the pelvis beside a hydrosalpinx showing the 'waist sign'. This patient presented with dull chronic pelvic pain, deep dyspareunia, and primary infertilty. She gave history of pelvic inflammatory disease in the past.
Despite the great value of transvaginal scan examination in diagnosing pelvic adhesions, diagnostic laparoscopy remains to be the best method for confirming their presence, and to assess their extent. However, care should be taken during this procedure in patients who had previous surgical interventions, or gave history of previous peritonitis. This is especially so during insertion of the needle and the trocar, as most injuries occur during these two initial steps. In such cases, Palmers point should be used first to create the pneumoperitoneum and for introducing the scope. The needle and trocar should be inserted just underneath the costal margin on the left side in the midclavicular line, lateral to the rectus muscle. A nasogastric tube in the stomach will also reduce the chances of it being injured during this procedure. Alternative sites can be selected afterwards under direct vision and used for repositioning of the scope, and for other operative equipment. It is important to emphasise the point that the majority of bowel injuries usually occur at the initial steps while introducing the needle and trocars, rather than during the intra abdominal operative procedures themselves.
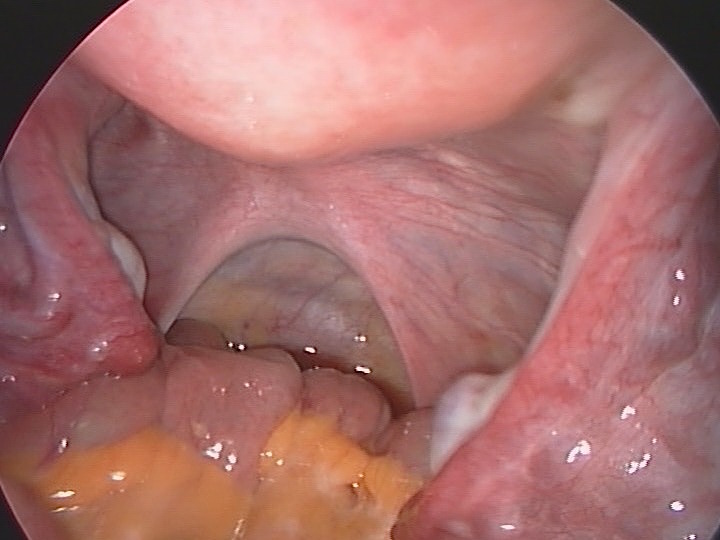
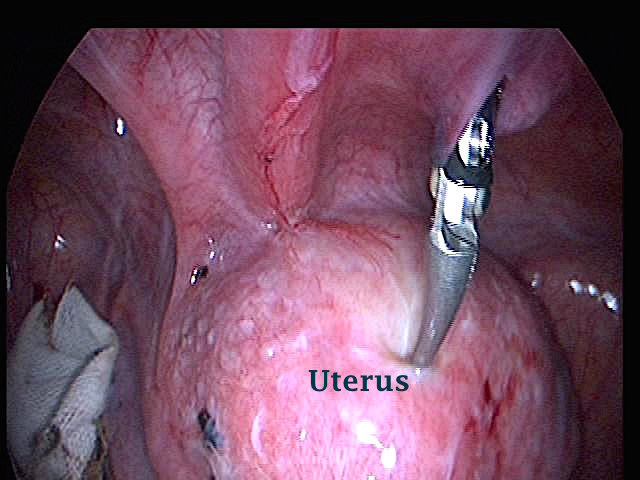
The first laparoscopic picture shown below revealed a healthy looking pelvis with no evidence of adhesions or endometriosis. Laparoscopy was done during the investigations of unexplained infertility in this case.
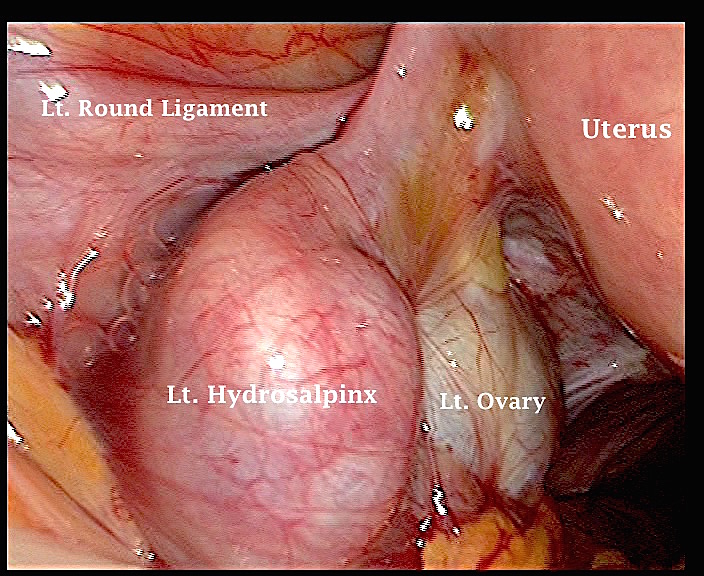
The second picture shows hugely dilated left hydrosalpinx, with the fimbrial end tethered to the upper pole of the left ovary. Part of the medial aspect of the left ovary is also seen, while the lateral aspect is attached to the pelvic sidewall. This patient tested positive to chlamydia, and gave history of recurrent pelvic inflammatory disease episodes in the past. Chronic pelvic pain and deep dyspareunia were the presenting symptoms.
Adhesions following surgery
Abdominal and pelvic surgical operations are followed by some adhesions formation in up to 94% of the cases [Becker et al, 1996]. Even common operations like a caesarean section, ovarian cystectomy or appendectomy could lead to extensive adhesions whether complicated by infection or not in the predisposed patient. This follows the normal healing response of the injured peritoneum which starts immediately after trauma. An acute inflammatory process leads to the formation of a fibrin matrix within few hours after surgery or any other form of trauma to cover the injured or inflamed area. However, this same protective mechanism is also responsible for adhesions formation within 48 hours. This was the basis why some attempts were made in the past to perform second look laparoscopy within few days after surgery to deal with all thin fibrinous adhesions before they became thicker and vascular. It is also important to remember that there is reduced fibrinolytic activity following peritoneal trauma secondary to reduction in tissue plasminogen activator and increased plasminogen activation inhibitor (PAI-1) levels [Holmdahl et al, 1996 and Holmdahl L, 1997]. Accordingly, the fibrin matrix would not resolve leading to adhesion formation between the injured surface and any adjacent tissues. This also forms the basis why some patients are more likely to develop adhesions than others after similar abdominal or pelvic surgery. Such patients were shown to have decreased levels of tissue plasminogen activator and increased expression of the PAI-1 activity [Holmdahl et al, 1998]. Adhesions are also more likely to involve the ovaries [Trimbos-Kemper et al, 1985] hence care should be taken when handling them. They also heal better without any resuturing. On the other hand rough handling of the tissues during surgery, foreign bodies like talcum, peritoneal reapproximation with suture material and low-grade infection have all been associated with increased risk of adhesions formation.
Over the years many ideas and procedures have been introduced to reduce the risk of postoperative adhesions formation including:
Microsurgical techniques and minimal access surgery to prevent tissue damage.
Continuous hydration to prevent tissue drying.
Limited use of monopolar energy.
Use of non absorbable sutures instead of absorbable ones.
Creation of artificial ascites by leaving some fluid in the abdominal cavity after surgery to keep the bowel afloat. Both crystalloid and non-crystalloid solutions have been used.
Use of both intraperitoneal or systemic anti inflammatory drugs and steroids.
Use of fluid or solid anti adhesion barrier agents.
None of these methods proved very effective in preventing postoperative adhesions formation though few of them might be more useful than others. Different meta-analyses have been published and they all agreed on the ineffectiveness of these methods. As an example, Watson et al (1999) reviewed randomised controlled trials performed to investigate the adjuvant effect of steroids, dextran 70, noxytioline, heparin or promethazine in preventing adhesions formation after pelvic surgery. None of these items except for steroids had any beneficial effect on adhesions recurrence or severity during second look laparoscopy. The evidence regarding the use of steroids was not conclusive either. A recent report by the Practice Committee of the American Society of Reproductive Medicine (ASRM) in 2006 stated that anti-inflammatory agents and peritoneal instillates had no verifiable benefit in preventing adhesions formation after surgery. On the other hand, a more recent review of published clinical controlled trials written by Ait Menguellet et al in 2007 demonstrated the safety and benefit of Interceed and Seprafilm in reducing postoperative adhesions formation. However, they found no sufficient evidence to recommend the use of other barrier agents. It is evident that there is no ideal method to prevent adhesions formation altogether. Accordingly, using microsurgical techniques during laparotomy or minimal access surgery would be the best options to use in all cases with or without any other barrier method which might prove significantly useful in the future. This entails minimal tissue damage, continuous tissue hydration, proper haemostasis and use of nonabsorbable suturing material. Laparoscopic surgery should be performed rather than laparotomy whenever possible, as it causes fewer postoperative adhesions [Mettler L, 2003]. However, the feasibility of this option would be controlled by many factors including the nature of the pathology itself and the endoscopic experience of the involved gynaecologist. Conversely, it should be appreciated that reduction in postoperative adhesions formation does not mean automatic enhancement of the fertility potential or elimination of postoperative bowel adhesions and pelvic pain. This point has been stressed by the ASRM practice report mentioned before.
The role of adhesiolysis in dealing with postoperative adhesions needs further discussions as adhesions usually form and pain usually starts within the first few months after surgery. Accordingly, delayed pain starting 12 months or so after the operative procedure is most unlikely to be related to adhesions. In such cases, more attention should be paid to other causes of pelvic pain and why the operation had been done in the first place as neuropathic pain might be an issue. This is the sort of scenario where a thorough psychological assessment is necessary before contemplating further surgery to deal with any adhesions. However, the situation might be different in cases of endometriosis and recurrent pelvic inflammatory disease which are progressive problems and the pattern of adhesions might change with time. It has also been known for more than 20 years that second look examinations usually showed formation of new adhesions and recurrence of older ones despite all the precautions mentioned before [Trimbos-Kemper et al, 1985; Raj and Hulka, 1982 and Tulandi et al, 1989]. Unfortunately, this remained to be the case today despite all the developments in surgical techniques and the frequent use of laparoscopic surgery. A recent review by Senthilkumar and Dreyer in 2006 confirmed a beneficial effect for adhesiolysis in relieving bowel obstruction and causing some improvement in the fertility potential but its role in the treatment of chronic pelvic pain was doubtful. This is mostly due to the fact that multiple factors are usually involved in causing chronic pelvic pain.
The first laparoscopic image above shows bowel herniated into a previous appendectomy scar. The patient presented with right side lower abdominal pains and persistent bloating sensation since having an appendectomy operation few years ago. Her symptoms improved dramatically following the release of the hernia and correcting the deficient scar.
The second image depicts almost 3/4 of the anterior surface of the uterus attached to the anterior abdominal wall. The patient presented with deep dyspareunea and secondary infertility, following two caesarean sections. The uterus was sitting high and could be felt abdominally. On the other hand, the cervix was very high up the vagina and could hardly be seen during speculum examination
The third image shows an frozen pelvis with bowel, omental, left tube and ovary and uterine adhesions amalgamated together. This patient had previous caesarean section with cervical stenosis and amenorrhoea postoperatively Most likely all menstrual blood over the period of amenorrhoea drained backward into the pelvis through the tubes. No endometriosis was found following painstaking release and excision of all these adhesions. This patient as well had chronic pelvic pain, deep dyspareunia and postcoital pain lasting for more than one day after intercourse
Adhesions following endometriosis
With endometriosis the site of pelvic adhesions depends on the site and extent of the disease. Significantly more moderate and severe adhesions were seen in patients with endometriomas and dysmenorrhoea (29.1%) compared to patients with endometrioma but no dysmenorrhoea (8.3%) as reported by Leng et al in 2007. This could be taken as a further proof confirming the role of adhesions in causing pelvic pain. The ovaries might also be stuck to the pelvis sidewall without any other obvious adhesions. Alternatively, the whole pelvis could be involved to different degrees. However, the fallopian tubes are usually patent but could have thick walls and restricted motility depending on the extent of the pathology. With rectovaginal endometriosis, only minimal adhesions could be present involving the rectum, back of the cervix and upper vagina. Feeling a nodule during vaginal and rectal examinations could be the only diagnostic clue possible. Accordingly, applying the modified American Society for Reproductive Medicine classification of adhesions would not be helpful in such cases.
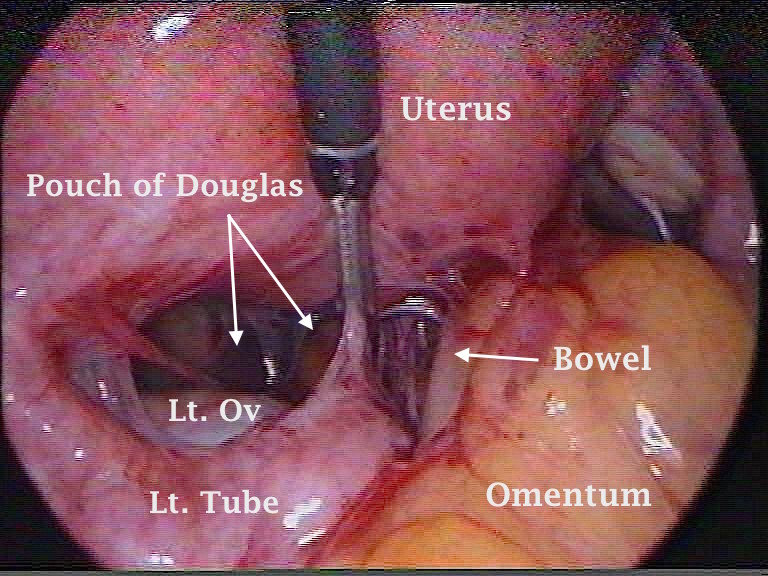
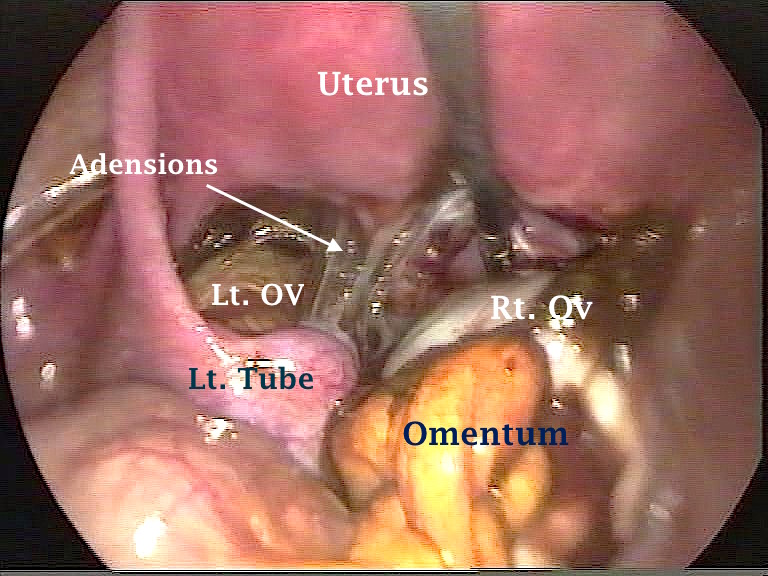
The first laparoscopic picture shown below demonstrates endometriotic pelvic adhesions in the pouch of Douglas involving the rectum. Such adhesions can cause rectal narrowing without involvement of the rectum itself with endometriosis. Excision of these adhesions may relieve any related symptoms without the need for any further surgery. The second picture shows pelvic adhesions caused by endometriosis involving the back of the uterus, ovaries tubes, omentum and pelvic sidewalls.
The first ultrasound image below shows two endometriotic cysts, deep in the pouch of Douglas.
The second laparoscopic image shown below depicts the two endometriotic cysts seen in the first image. Note that both ovaries, tubes, omentum, bowel and back of the uterus were all involved in a large coagulum occupying the pouch of Douglas.
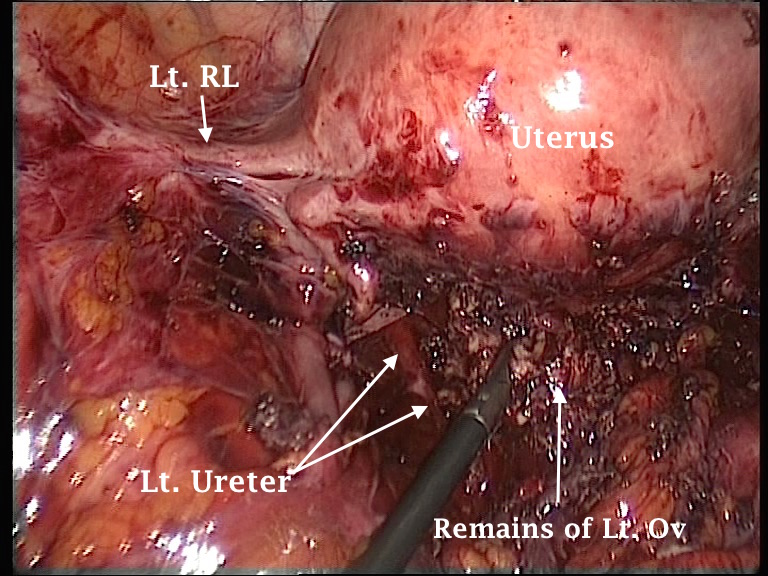
The third image shows severe pelvic adhesions with complete obliteration of the pouch of Douglas. The left ureter had to be dissected extraperitoneally. It can be seen lateral to the remains of left ovary endometriotic tissue. This had to be removed piecemeal to clear the pouch of Douglas. This last patient's presentation was very severe, almost constant pelvic pain, dysmenorrhoea, dyspareunea and dyskesia.
Formation or recurrence of adhesions after surgical treatment of endometriosis has been studied by Parker et al in 2005. In general, more adhesions were seen during second look laparoscopy when adhesions with or without underlying endometriotic lesions were removed than in cases when only endometriotic lesion without overlying adhesions had been excised, during the first surgical procedure. Furthermore,there was more significant recurrence of thick adhesions and those involving the ovaries than thin ones and those involving the tubes or ovarian fossa, respectively.
To reduce the recurrence of postoperative ovarian adhesions after endometriotic surgery, Ouahba et al (2004) suggested transient unilateral or bilateral ovariopexy to the anterior abdominal wall. They did not find any further reformation of adhesions during second look examinations in 66% of the ovaries initially involved with adhesions and severe endometriosis after using this technique.
Final remarks about adhesions irrespective of their cause
It is very difficult to find identical prospective studies or review articles addressing the same factors related to or associated with pelvic pain and adhesions formation reaching the same sort of conclusion. Accordingly, two questions still remain to be answered:
Do adhesions cause chronic pelvic pain?
Is adhesiolysis effective in relieving chronic pelvic pain?
The subjects of pelvic adhesions and chronic pelvic pain are complicated by many confounding factors and before any meaningful answers could be given, the following points should be addressed first in each individual case to help with decision making:
What was the initial cause of the pelvic adhesions?
Which organs are involved with these adhesions and to what extent?
Are we dealing with thin or thick adhesions?
Is there an active background progressive pathology like endometriosis or PID or are they stand alone mature adhesions following surgery?
Is there a fertility issue on top of chronic pelvic pain?
Would adhesiolysis be necessary before another definitive surgical procedure could be done?
Has adhesiolysis been attempted before?
How much of the pain is related to the adhesions or to another underlying cause and how much of it has already become neuropathic?
What is the psychological predisposition of the patient and her pain threshold?
It has already been found that identifying and dealing with a single pelvic pathology would most likely be unsuccessful in treating chronic pelvic pain [Butrick CW, 2007] as it is usually caused by many pain generators. This statement is valid for adhesiolysis as it deals only with pelvic adhesions while other pain generators might not be addressed at the same time. The following answers could be given bearing in mind all these factors and the information given under the different sections related to adhesion caused by endometriosis, surgery and PID.
The evidence available now confirms the fact that adhesions could cause different types of pelvic pain especially if the bowel is involved or if they are associated with endometriosis or PID. Furthermore, ovarian adhesions with endometriomas have been shown to cause more pain than isolated endometriomas [Leng et al, 2007]
Adhesiolysis is not useful for the total abolition of chronic pelvic pain in many cases as it is mostly caused by many factors rather than one cause. However, it could give transient pain relief but recurrence of both adhesions and pelvic pain is usual. Nevertheless, it could be effective in reducing pain intensity if it has been combined with such procedures as excision of rectovaginal or uterosacral endometriosis. It is also effective to different degrees in relieving intestinal obstruction.
One can also give the following additional points for consideration:
Treatment of bowel adhesions to anterior abdominal wall gives pain relief.
Mobilisation of the ovaries also reduces pain intensity.
Treatment of endometriomas involved with adhesions gives more pain relief than treatment of endometriomas not involved with adhesions.
Adhesions recur more readily after treatment of endometriosis involved with adhesions than treatment of endometriosis alone or adhesions alone. This emphasises the role of the underlying pathology in causing adhesions
Thick adhesions recur more readily than thin adhesions.
On a different note, adhesiolysis may help in improving the fertility potential of many patients, so long as there was no significant tubal damage. Successful outcome has been shown to be inversely related to the severity of the adhesions. The risk of ectopic pregnancies can be increased in such cases.
This section can be concluded by stating that prevention of postoperative adhesions formation is only possible by stopping all surgical operations. Since this is not a viable option, unnecessary interventions should be avoided and preventative measures to reduce adhesions formation should always be implemented, irrespective of the type of the surgical procedure performed. Furthermore, each case should be considered separately in a risk / benefit assessment protocol before making any decisions whether to operate or not to operate in patients with pelvic adhesions.