Fibroids
Though fibroids are historically included as one the causes of pelvic pain they are rarely a cause of the chronic type. They were not included in a list of 60 risk factors associated with chronic pelvic pain, dysmenorrhoea or dyspareunia in a recent review reported by Latthe et al in 2006. However, within every day clinical practice they may occasionally be associated with dysmenorrhoea. This may be secondary to the related excessive bleeding and clots expulsion, or due to adenomyosis or endometriosis which are commonly associated with fibroids. Ferrero et al (2006), in a more direct approach, found no significant effect of fibroids number, size or position on the prevalence or intensity of chronic pelvic pain. Furthermore, there was no correlation between the prevalence or severity of deep dyspareunia or sexual dysfunction and fibroids. Degeneration of fibroids can be another cause of pain but this is usually an acute episode. It is more common during pregnancy and pain may last for a long time in such cases. More information will be given about fibroids in chapter 2.
Chronic endometritis
Chronic endometritis can cause some pain and irregular uterine bleeding. It may be seen in 3 - 10% of endometrial biopsies retrieved from women with abnormal uterine bleeding. Though it may not be a common presentation in women with chronic pelvic pain, it must be kept in mind especially in patients who had intrauterine intervention or those wearing an intrauterine contraceptive device. Pyometra may be seen in older women and those with cervical stenosis.
Histological diagnosis of chronic endometritis depends on the presence of plasma cells in the endometrial biopsy. Other diagnostic features include superficial stromal oedema and increased lymphocytes and leucocytes infiltration. Occasionally, difficulty may be encountered in identifying plasma cells with routine H and E staining. In such cases additional techniques may be useful, including methyl green pyronin stain and immunohistochemistry for immunoglobulin G.
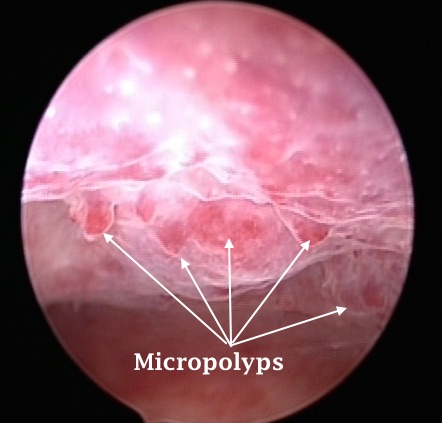
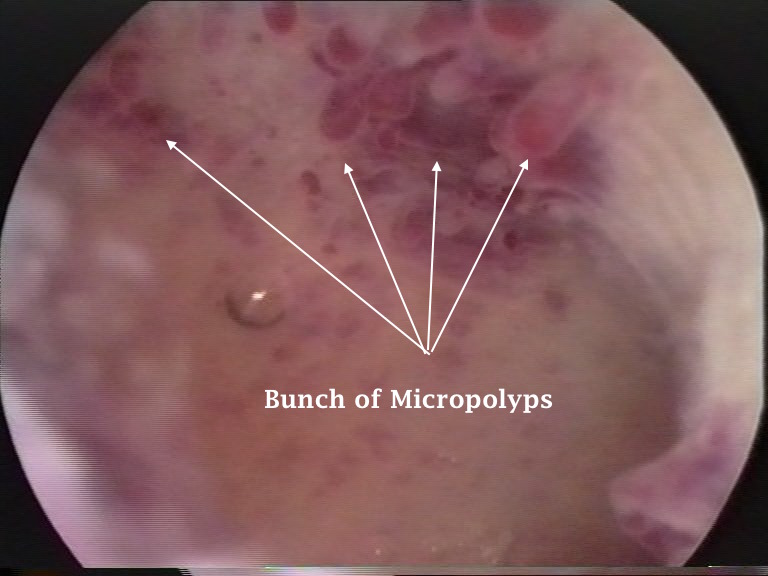
With the current surge in using diagnostic hysteroscopy, the presence of endometrial micropolyps has been identified as a diagnostic feature of chronic endometritis. This is valid only with fluid hysteroscopy, and not with the CO2 technique. Conversely, absence of micropolyps does not exclude the diagnosis.
The two hysteroscopic images depicted above show micropolyps, which are diagnostic of chronic endometritis. Each micropolyp is one mm tall, and are usually found in groups, which made them more conspicuous in these two cases. They are not usually seen during transvaginal scanning, but small thickened focal areas may give clues to their presence in patients with abnormal uterine bleeding, chronic pelvic pain and abnormal vaginal discharge.
Intrauterine contraceptive devices
Both cupper and levonorgestrel loaded devices have been used more frequently in recent years. The mirena device is usually used both for contraception, and for control of excessive menstrual blood loss. The commonest presentation of patients using such devices in the pain clinic is dysmenorrhoea, which usually settles with time. Except for the mirena device, heavy periods with clots can be a problem. More serious complications are related to dislocation of the device or perforation of the uterine wall. Intrauterine contraceptive devices have been found in the bladder, rectum and anterior abdominal wall by different authors. In such cases the device should be removed, even if the patient has no related symptoms. Occasionally, pain and bleeding are related to pelvic infection while using an IUCD. Chlamydia should be kept in mind in younger age groups.
On the other hand insertion related pelvic infection is 6-fold higher during the first month after the device insertion. Thereafter, the risk is affected by factors which are known to increase PID risk even without using such devices. The list includes young age, multiple partners, not using condom, attitude of male partners and prevalence of sexually transmitted disease in that society [Meirik, 2007].
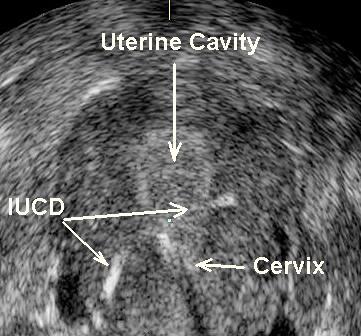
- The first 3D ultrasound image shown above depicts a uterus with an IUCD which has perforated through the caesarean section scar. She gave history of difficult IUCD insertion and presented with lower abdominal pain and blood stained vaginal discharge.
- The second 2D ultrasound image above shows both the uterine cavity and left fallopian tube filled with pus. The patient presented with general ill health and lower abdominal pain.