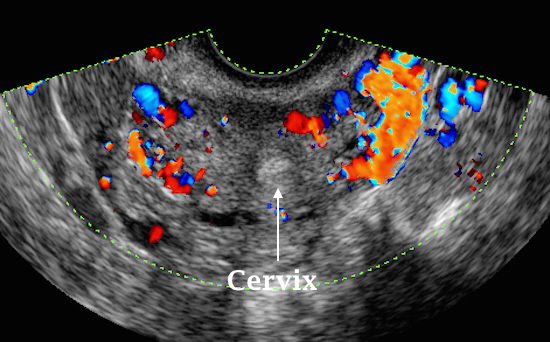
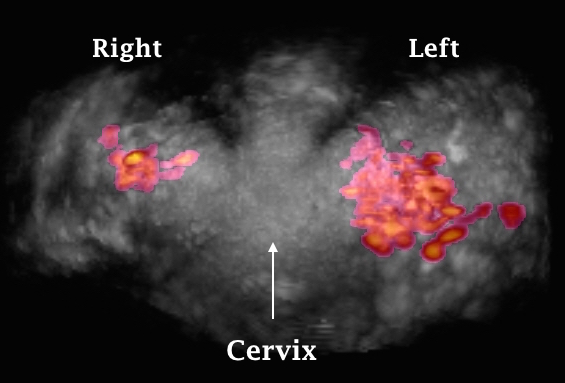
The two ultrasound images shown above demonstrate increased vascular marks in the left broad ligament compared to the right side in two patients examined with 2D colour Doppler and 3D power Doppler respectively.
Pelvic congestion may also be seen during
laparoscopic examination, especially in the broad and infundibulopelvic
ligaments. However, previous reports showed no correlation between venography
and the findings during laparoscopy. This may be due to the modulating effect
of the head down position and increased intra abdominal pressure sustained
during laparoscopy.
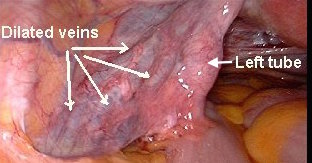
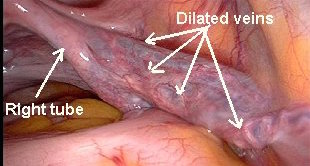
The two laparoscopy pictures shown below depict pelvic congestion of the broad ligaments during laparoscopy. Congestion on both sides was very evident despite the patient being in 30º Trendelenburg position
Management of pelvic congestion syndrome
Despite the
long duration of time since this diagnosis was first described, no specific
treatment has yet been agreed upon. This could be a reflection of the general
hesitancy by gynaecologists to accept even the existence of the pathology
itself. However, both medical and surgical means have been described with
variable results.
Medical treatment
Medroxyprogesterone
acetate (MPA) in a daily dose of 30 mg for 6 months has been shown to cause
temporary symptomatic relief as well as reducing the size of the dilated
vessels themselves. One study reported such an effect in 77% of the patients so
treated. However, suppressing ovulation with the oral contraceptive pills
failed to give similar symptomatic relief suggesting a direct antioestrogenic
effect by MPA on the blood vessels. Unfortunately, this was a short-term remedy
which lasted only while using the drug [Kroon and Reginald,
2005].
Dihydroergotamine has also been used but there is no enough general experience
with it as for medroxyprogesterone acetate. Furthermore, downregulation with
monthly injections of a GnRH analogue provided symptomatic relief, improved
sexual function and reduced anxiety and depressive states [Kroon and
Reginald, 2005]. On the other hand, Simsek et al in 2007 showed
that 3 months use of Daflon, which is a venomimetic agent capable of regulating
the circulatory venous tone, resulted in significant reduction in the frequency
and severity of symptoms. They concluded that pharmacological augmentation of
venous tone could improve the pelvic circulation and relieve patients
symptoms.
Surgical treatment
Different surgical
techniques have been used in the management of pelvic congestion syndrome
including ovarian vein ligation, hysterectomy with or without removing the
ovaries and tubes. Ovarian veins ligation was successful in giving symptomatic
relief in only 50% of the cases whereas hysterectomy was not successful unless
combined with bilateral salpingo-oophorectomy. Another surgical technique which
gave some favourable response is correction of uterine retroversion by
shortening of the uterosacral ligaments. Catheter embolisation of the ovarian
veins is proving at least as effective as surgery for relieving patients
symptoms. Maleux et al [2000] reported 58.5%
total relief of symptoms where as Kim et al [2003] reported
83% clinical improvements at long term follow up. The last figure is almost
identical to the one reported by Kwon et al in 2007
after ovarian vein embolisation using coils. This dramatic improvement in the
reported results over the years might indicate improvement in the technical
abilities of the intervention radiologists with time.
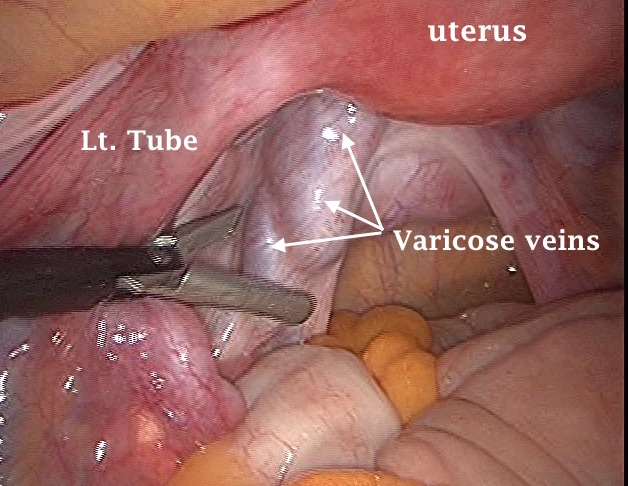
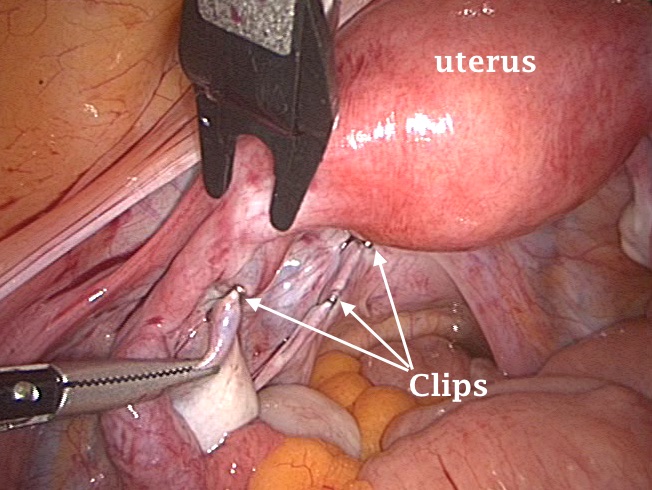
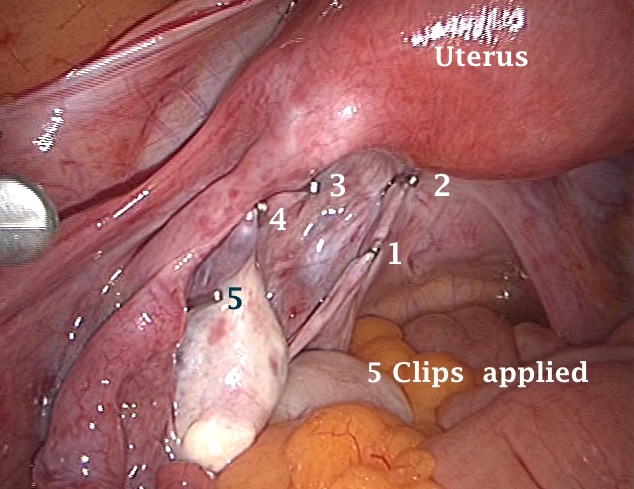
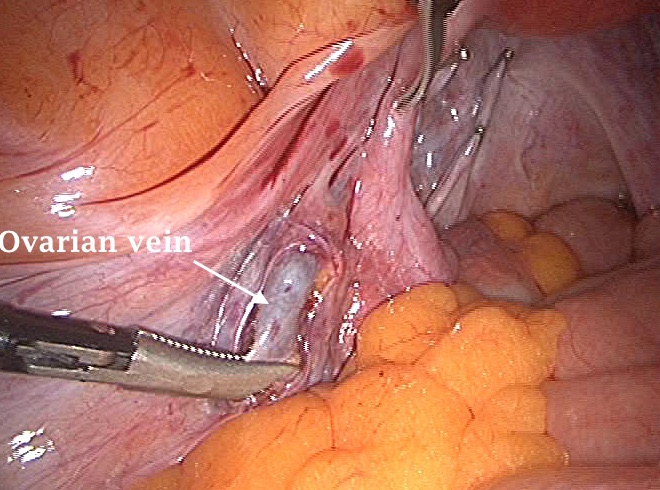
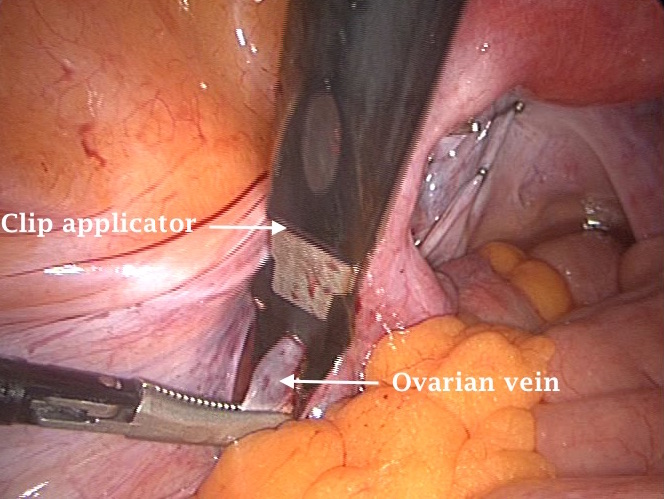
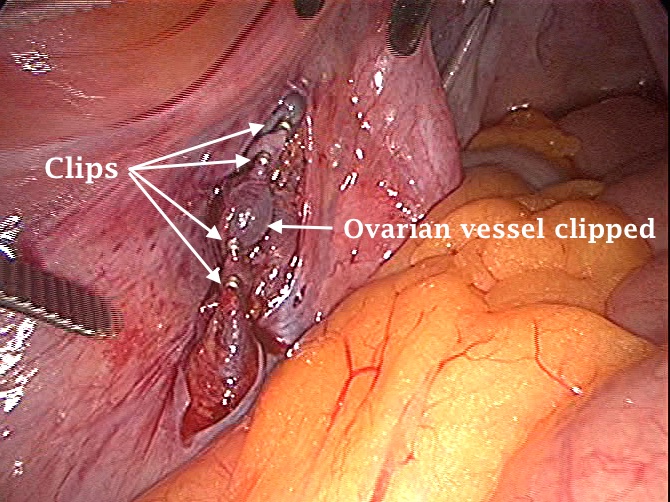
The 6 photographs shown
above demonstrate left pelvic sidewall varicose veins dissected and clipped.
Only few of the clips are shown in these photographs. Varicosity can be
seen lateral to the left uterosacral ligament, pelvic sidewall, the left broad ligament and lateral to the infundibulopelvic
ligament. The patient had chronic pelvic pain with no other demonstrable cause.
Ultrasound scan examination revealed left side pelvic congestion which did not
respond completely to high doses of medroxyprogesterone acetate for a period of 6 months. Her symptoms,
mainly deep dyspareunia and postcoital pain, subsided for one year after
surgery. The patient was lost to follow up afterwards. Despite the good success with this case, it does not mean that such a procedure will be equally successful in all other similar cases.